
.png)
Key Takeaways:
- Excessive, one-size-fits-all training stalls startup, squanders site hours, and drives the deviations it’s meant to prevent
- The fix isn’t less training; it’s mindful training and precision guidance, delivered by role, on-demand, and throughout the study
- Five honest questions will tell you whether your training is part of the solution or part of the burden
You might not know it, but there’s a high chance excessive clinical trial site training requirements are stalling your study startup, increasing site burden, and creating inefficiencies that lead to delays, deviations, and higher study costs.
This is precisely why SCRS launched the Cut 25 initiative to reduce redundant or inefficient site training requirements by 25%. It’s a real commitment to a real problem. But it also poses a tough question: Can your current training approach actually get you there?
The data says probably not...
- Sites are spending 15 to 20 hours per month, per trial, just on technology training.
- Turnover is running as high as 61%.
- And more than 90% of protocol deviations trace back to training gaps.
 Knowing the model is broken and knowing what to replace it with are two very different things. So instead of a prescription, here are five questions.
Knowing the model is broken and knowing what to replace it with are two very different things. So instead of a prescription, here are five questions.
Answer honestly! Otherwise, you’ll never know if your training is a part of the solution or a part of the burden it’s trying to fix.
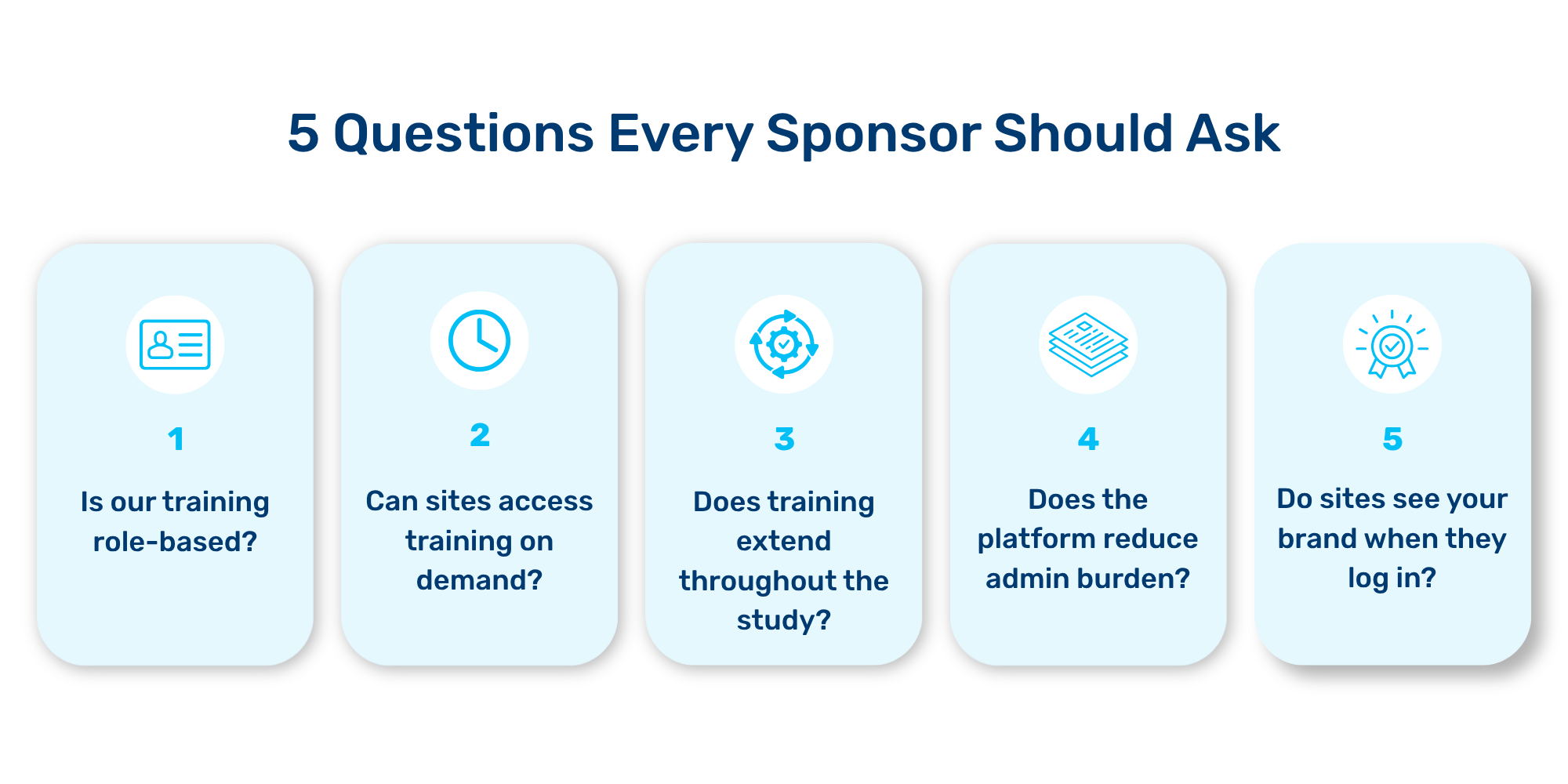
5 Questions to Ask About Your Site Training
#1: Is our training role-based, or does everyone sit through the same session?
A principal investigator and a research coordinator do not need the same training. A site in Tokyo has different regulatory requirements than a site in Toronto. An experienced coordinator who’s run five oncology trials doesn’t need the same walkthrough as someone on day one of their first study.
But the baffling truth is that most sponsors still deliver training as a single session that treats everyone identically. Same slide deck. Same length. Same level of detail. Whether you’ve done this a hundred times or never. Whether it’s specific to your role or not.
That’s not training. That’s a formality.
Sponsors can cut training time significantly for experienced staff simply by not wasting their time on content they don’t need. Platforms that let sponsors filter content by role, site, country, and study help to ensure each person sees only what’s relevant to their actual responsibilities.
Ask yourself: Can your training platform tell the difference between a coordinator, a sub-investigator, and a pharmacist? Or does everyone get the same 90-minute session and a pat on the back?
#2: Can sites access training and resources on demand, or only through the LMS system?
The one-and-done model is built on hopes and dreams that almost never hold up: that every coordinator will remember everything weeks or months later, that CRCs will not turn over between the investigator meeting and the first patient, and that the protocol won’t change.
The person you trained at the SIV may be gone before enrollment starts. Their replacement needs to get up to speed fast, but the live session they missed isn’t coming back. And when FPI is in April but visit 12 isn’t until September, forcing someone to sit through detailed visit 12 training in February is a waste of everyone’s time. They’re not going to remember it. You know that. They know that.
What does work is on-demand access. Documents, short videos, and integrated visit workflows available the moment the coordinator needs them, in the format that fits the content. (Pro tip: training doesn’t have to be done in PowerPoint!)
Ask yourself: If a new coordinator joins mid-trial, how do they get trained? Is there an on-demand library organized by visit and role? Or do they wait for the next scheduled session? Or worse yet, do they learn the protocol on their first patients?
#3: Does training extend throughout the study, or does it end at startup?
Most site training happens at two events: the investigator meeting and the SIV. Then it stops.
But the trial sure doesn’t stop. Protocols evolve, time elapses between visits, other studies get onboarded, staff rotate. The coordinator preparing for visit 12 in 8 months is operating in a completely different context than the person who sat through the SIV.
When training ends at startup, sites quickly forget. The result is unsurprisingly ugly. Coordinators test drive the protocol on their first few patients through trial and error, when they should be executing with guidance. That’s how you get protocol deviations (which, ironically, are exactly what training was supposed to prevent!).
Consider the alternative: visit-level guidance that runs throughout the study. When a coordinator preps for a specific visit, the relevant procedures, reminders, and references from all the documents (protocol, lab, pharmacy manual) are right there. Training evolves from a one-time event to an ongoing operational support system.
Ask yourself: When a coordinator sits down to prep for visit 8 on a Tuesday morning, can they pull up the specific procedures and forms for that visit? Or are they scrolling through a recording from four months ago, hoping to find the right section?
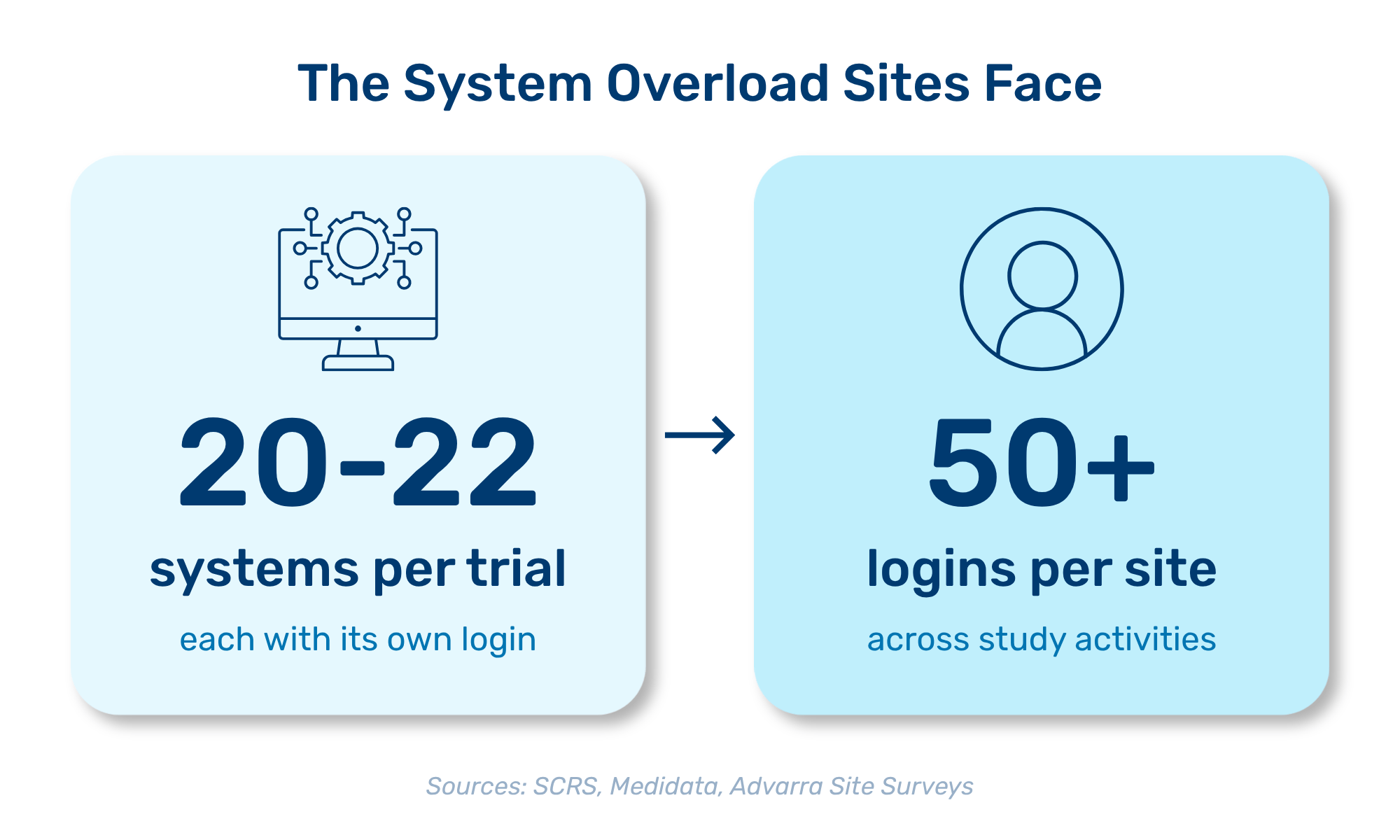
#4: Does our training platform reduce admin burden, or add to it?Let’s take a good, hard look at the numbers. Sites today manage 20 to 22 different systems per trial. Across multiple active studies, that’s 50+ logins. Every new vendor and every new sponsor piles on another portal, another training requirement, and another set of credentials. Yet even when sites already know the system, they still have to sit through the training again for each new study.
The administrative pain doesn’t end there. Training completion records need to end up in the eTMF. When training and the eTMF live on separate platforms, someone has to manually upload certificates, chase down completions, and track gaps.
When training documentation is powered by an eTMF integration, compliance documentation takes care of itself. Completion records flow straight into the trial master file. Real-time dashboards show who’s trained and who isn’t, before a monitoring visit surfaces the problem, not during one.
Ask yourself: Does your training platform auto-file completion records to the eTMF? Can you see real-time completion status across all sites right now, or do you find out about gaps when the monitor flags them?
🔍 Learn more about how ProofPilot’s Staff Training solution actually reduces the burden on site staff.
#5: When sites log in, do they see your brand, or someone else's?
This sounds cosmetic, but it's not.
When a site logs into a training portal and sees a third-party vendor’s logo, they’re not entirely sure who they’re working for. Now multiply that across 20 active studies, each with different CRO platforms and vendor portals. Things get confusing, fast.
And when training runs through a CRO’s platform, there’s a structural problem that no amount of good intentions can fix. CRO platforms serve multiple sponsors, which means they can’t eliminate duplicate training across studies. That redundancy is baked in by design.
Sponsor-branded training changes the equation. Sites log in and see the study name with the sponsor’s logo/colors/visuals, creating a consistent experience across documents, chat, and training. This reduces confusion and builds trust. That matters when you’re competing for the same site’s attention as every other study.
Ask yourself: Is your training experience branded as yours, or does the site see another vendor’s logo when they log in?
The Answers Tell the Story
If you answered “no” to most of these, it doesn’t mean your team doesn’t care about training. It simply means the tools you’re relying on weren’t built for today’s reality: high turnover, multiple concurrent studies, complex protocols, and sites drowning in systems.
But here’s the blunt truth: Cut 25 was not intended to tackle an unsolvable problem. It’s to provide best practices for a sponsor decision. Sites can’t fix the training they’re given. They can only endure it. The power to change sits with the sponsors who pick the tools, define the content, and decide whether training is a compliance checkbox or something that actually helps sites run the study right.
Ready to explore a great tool for this? Learn more about Staff Training.
Your next read: What Cut 25 Actually Takes
Explore what it takes to actually reduce the training burden for your sites. Read our deep dive: Cutting Clinical Trial Site Training Burden by 25%.
Research Site Training FAQ
Why is role-based training important for clinical trial sites?
Different roles within a clinical trial site have distinct responsibilities. Tailoring training to specific roles ensures that personnel receive only the information relevant to their tasks, enhancing retention and application of knowledge.
How does on-demand training benefit clinical trial sites?
On-demand training and guidance support just-in-time learning by allowing clinical trial site staff to access training materials and resources whenever they need them. This helps new staff onboard more quickly and provides ongoing support as protocols evolve throughout the trial.
What administrative burdens do clinical trial sites face with current training methods?
Sites often manage multiple systems per trial, each requiring training completion tracking, managing different vendor portals, and correctly filing compliance documentation in the eTMF. Efficient training platforms that automate these processes help reduce the time spent on administrative tasks.



%201.svg)

